
Leading the revolution in pancreatic cancer
Home / Our therapy areas / Oncology / Leading the revolution in pancreatic cancer
Pancreatic cancer is the 4th leading cause of cancer death in western countries and the 7th leading cause of cancer death globally, largely due to the complexities in its biology and management.1,2,3 It also has one of the worst survival rates of all ‘common’ cancers, with only 9% of patients with advanced (metastatic) disease surviving more than five years after diagnosis.4 Pancreatic ductal adenocarcinoma (PDAC) is the most common form of pancreatic cancer (accounting for 85% of cases)5, compared with pancreatic neuroendocrine tumours (PNETs) which are far less common and account for around 4% of cases.6
PDAC is one of the most aggressive forms of cancer.7 Due to the diversity of genetic mutations and dense connective tissue that forms the pancreas, PDAC is also one of the most chemo-resistant and radio-resistant type of cancer.1,8 PDAC has an extremely poor prognosis with only ~20% of patients surviving one-year at all stages of the disease.9 The causes of pancreatic cancer are still not well understood, although certain risk factors such as smoking, diabetes, obesity and chronic pancreatitis have been identified.2
Thanks to dedicated scientific research, there have been positive developments to better manage this high morbidity cancer. To understand why pancreatic cancer presents such an intricate and complex challenge, we must first understand the crucial role that the pancreas plays in regulating bodily functions.
The pancreas – bringing balance to the body
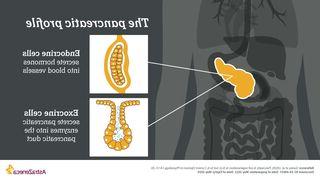
The pancreas itself is a gland organ located in the abdomen near the liver. The pancreas plays a dual role in regulating bodily functions10,11:
- Endocrine system – the pancreas secretes hormones, including the blood sugar-regulating hormones insulin and glucagon, directly into the blood
- Exocrine system – the pancreas secretes enzymes into the digestive tract through a duct into the duodenum, which is responsible for breaking down food and absorbing nutrients.
Pancreatic tumours
Pancreatic cancer is classified into two main tumour types – depending on whether the tumour forms in the exocrine cells, or in the endocrine cells.
PNETs, also commonly known as ‘islet cell tumours’, are a rare type of cancer that form in the endocrine cells.12 PNETs have a better prognosis, compared to more common types of cancer.10
Exocrine tumours account for 96% of pancreatic cancers and is most commonly PDAC.5,13 PDAC develops from the cells which line the ducts in the pancreas. These ducts carry the digestive juices, containing enzymes, into the main pancreatic duct and then into the first part of the small intestine.9
As this disease has the potential to spread quickly and symptoms often do not present until the disease is at an advanced stage, more than 50% of pancreatic cancer patients are diagnosed when the disease has already spread to other organs in the body – for these patients the average survival is less than one year.5,14
There are multiple reasons for the potentially quick spread of this disease, including the close proximity of major blood vessels in the pancreas, which can be readily invaded by cancer cells.15 As PDAC symptoms are non-specific, diagnosis is extremely challenging, which significantly reduces the chances of survival. This has led to PDAC being known as a ‘silent killer.’16

A limited treatment landscape highlights urgent unmet need
Historically, patients with advanced pancreatic cancer have faced poor outcomes due to the aggressive nature of the disease and limited treatment advancements compared to other tumour types, particularly lagging behind other common cancers with regards to precision therapy.2,4,17,18
Only approximately 20% of patients with advanced disease are eligible for surgery, due to the metastatic (advanced) stage of their cancer at the time of diagnosis, while treatment options including chemotherapy and radiotherapy are often limited.19,20 The high burden of symptoms in advanced pancreatic cancer presents further challenges, as symptoms can interfere with treatment efficacy and quality of life.21
Pancreatic cancer – is it possible this difficult disease could be biomarker-driven?
We have already come a long way in understanding what biomarker status means for cancers such as breast, prostate, ovarian, lung and gastric, to name a few. With the emergence of genomic profiling technologies, and selective molecular targeted therapies, biomarkers have now been shown to play an increasingly important role in the clinical management of pancreatic cancer patients.22
In PDAC, some tumour suppressor genes (which actively prevent the formation of cancer) are commonly mutated resulting in aggressive tumour growth.23 These genes, including BRCA1/2, PRSS1 and CDKN2A, are just some of the predictive biomarkers for metastatic pancreatic cancer, and have uses far beyond diagnosis; they may also be used to predict potential treatment outcomes and help identify familial risk of developing PDAC.5,24
Targeted cancer therapies are drugs that interfere with specific molecules involved in cancer cell growth and survival. To understand how targeted treatments work, it’s important to understand the mechanisms of cancer cells.25
The BRCA1/2 genes form part of the DNA damage response (DDR), or a process through which various pathways work to repair DNA damage. When the BRCA genes are mutated, the DDR repair process is hindered, and the risk of developing cancer increases.26 Around 5-10% of patients with familial PDAC and 3% of patients with sporadic PDAC are predicted to harbour a germline BRCA mutation. Knowing whether a patient carries this mutation may be used to help identify suitable treatment options.27
Cancer cells have high levels of DNA damage, loss of one or more DNA repair pathways increased DNA replication stress. These properties may be exploited as potential therapeutic targets. By researching agents that can target these particular dependencies, treatments may actively target a fundamental feature of cancer cells and turn this against itself, resulting in cancer cell death.27
For more information on exploiting cancer-specific DDR-dependencies click here
The future for pancreatic cancer research and development
The prevalence of pancreatic cancer will continue to increase if we do not achieve further breakthroughs in diagnosis and treatment. Current strategies to improve treatment outcomes focus on earlier detection through screening and biomarker testing with more effective, targeted treatments.28,29
BRCA-mutated metastatic pancreatic cancer is a devastating difficult-to-treat disease with critical unmet needs, but with ongoing innovation in genetic testing, the use of biomarkers, potential targeted therapies and continuous research, we are making progress in helping to change patients’ prognoses.30 AstraZeneca is committed to driving this progression and we strongly believe that to increase the pace at which progress is made in pancreatic cancer survival, we must push forward as a community to help raise awareness of unmet needs, and to activate change where we know improvements can be made.
References
- Zeng S, et al. Chemoresistance in Pancreatic Cancer. Int J Mol Sci. 2019 Sep; 20(18): 4504.
- Rawla P, et al. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J Oncol. 2019 Feb; 10(1): 10–27.
- Sung H, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 countries. (2021). CA Cancer J Clin. 2021 May;71(3):209-249.
- Tiriac H, et al. Organoid Models for Translational Pancreatic Cancer Research. Curr Opin Genet Dev. 2019 Feb;54:7-11.
- Tonini V, et al. Pancreatic cancer in 2021: What you need to know to win. World J Gastroenterol. 2021 Sep 21;27(35):5851-5889.
- Pancreatic Cancer UK. Pancreatic neuroendocrine tumours (PancNETs). Available at http://www.pancreaticcancer.org.uk/information/just-diagnosed-with-pancreatic-cancer/pancreatic-neuroendocrine-tumours-pancnets/. Accessed May 2022.
Pancreatic Cancer Action Network. Pancreatic Neuroendocrine Tumors (PNETs). Available at http://www.pancan.org/facing-pancreatic-cancer/about-pancreatic-cancer/types-of-pancreatic-cancer/endocrine-pancreatic-neuroendocrine-tumors/. Accessed May 2022. - Truong L, et al. Pancreatic Cancer Microenvironment and Cellular Composition: Current Understandings and Therapeutic Approaches. Cancers (Basel). 2021 Oct 8;13(19):5028.
- Chen S, et al. The synergistic tumor growth-inhibitory effect of probiotic Lactobacillus on transgenic mouse model of pancreatic cancer treated with gemcitabine. Scientific Reports. 2020;10:20319.
- Siddappa P, et al. Sa1375 – The Utility of Ca 19-9 in Patients Undergoing Eus for Pancreatic Ductal Adenocarcinoma: Single Center Experience Over 2 Decades. Gastroenterology. 2019;156;(6)1:331-332.
- American Cancer Society. (2020). What is a pancreatic neuroendocrine tumor? Available at http://www.cancer.org/cancer/pancreatic-neuroendocrine-tumor/about/what-is-pnet.html. Accessed May 2022.
- Britannica. Duodenum. Available at http://www.britannica.com/science/duodenum. Accessed May 2022.
- Pancreatic Cancer Action. Pancreatic Neuroendocrine Tumours. Available at http://pancreaticcanceraction.org/about-pancreatic-cancer/what-is-pancreatic-cancer/pancreatic-neuroendocrine-tumours/. Accessed May 2022.
- Pancreatic Cancer UK. Types Of Pancreatic Cancer. Available at http://www.pancreaticcancer.org.uk/information-and-support/facts-about-pancreatic-cancer/types-of-pancreatic-cancer/. Accessed May 2022.
- Azar I, et al. Treatment and survival rates of stage IV pancreatic cancer at VA hospitals: a nation-wide study. Journal of Gastrointestinal Oncology. 2019;10(4):703-711.
- McGuigan A, et al. Pancreatic cancer: A review of clinical diagnosis,epidemiology, treatment and outcomes. World Journal of Gastroenterology. 2018;24(43):4846-4861.
- Medical University of South Carolina. Pancreatic Cancer: The Silent Killer. Available at http://muschealth.org/medical-services/geriatrics-and-aging/healthy-aging/pancreatic-cancer. Accessed May 2022.
- Roth MT, et al. Recent advances in the treatment of pancreatic cancer. F1000Research. 2020;9(131):1-7.
- Regel I, et al. Current Strategies and Future Perspectives for Precision Medicine in Pancreatic Cancer. Cancers. 2020;12(4):1042.
- Guidelines Live. Pancreatic cancer: GPs can help prognosis by identifying early signs. Guidelines in Practice. Available at www.guidelinesinpractice.co.uk/cancer/pancreatic-cancer-gps-can-help-prognosis-by-identifying-early-signs/352855.article. Accessed May 2022.
- Niesen W, et al. Surgical and local therapeutic concepts of oligometastatic pancreatic cancer in the era of effective chemotherapy. European Surgery. 2019;51:153–164.
- Gilbertson-White S, et al. Understanding Symptom Burden in Patients With Advanced Cancer Living in Rural Areas. Oncology Nurse Forum. 2019;47(3):305-317.
- O’Neill RS, et al. Biomarkers in the diagnosis of pancreatic cancer: Are we closer to finding the golden ticket? World J Gastroenterol. 2021;27(26);4045-4087.
- Wang S, et al. The molecular biology of pancreatic adenocarcinoma: translational challenges and clinical perspectives. Signal Transduction and Targeted Therapy. 2021;6(249):1-23.
- Zhan W, et al. Germline Variants and Risk for Pancreatic Cancer: A Systematic Review and Emerging Concepts. Pancreas. 2018;47(8):924-936.
- National Cancer Institute. Targeted Therapy to Treat Cancer. Available at http://www.cancer.gov/about-cancer/treatment/types/targeted-therapies. Accessed May 2022.
- Huang R, et al. DNA damage repair: historical perspectives, mechanistic pathways and clinical translation for targeted cancer therapy. Signal Transduction and Targeted Therapy. 2021;6(254):1-35.
- Blair A, et al. BRCA1/BRCA2 Germline Mutation Carriers and Sporadic Pancreatic Ductal Adenocarcinoma. J Am Coll Surg. 2018 Apr; 226(4): 630–637.e1.
- Yang J, et al. Early screening and diagnosis strategies of pancreatic cancer: a comprehensive review. Cancer Communications. 2021;41:1257-1274.
- Aslan M, et al. Targeted Therapies for Pancreatic Cancer and Hurdles Ahead. Anticancer Research. 2018;38:6591-6606.
- Rosen M, et al. BRCA mutated pancreatic cancer: A change is coming. World J Gastroenterol. 2021;27(17):1943-1958.