
Ovarian Cancer
Augmenting our commitment in ovarian cancer
Home / Our therapy areas / Oncology / Ovarian Cancer
Ovarian cancer is a devastating disease which affects the primary reproductive organs for females. At birth the ovaries are rendered as body tissue, until very sophisticatedly, once a female reaches puberty and matures physically, so do her ovaries.1,2
Despite advances in treatment, ovarian cancer is one of the most common female cancers3 and the eighth most common cause of death from cancer in women worldwide.4 The goals of front-line therapy have always been to delay progression of the disease for as long as possible and maintain the patient’s quality of life with the intent of achieving complete remission - yet currently ~70% of patients relapse within three years of initial treatment.5,6,7,8
These statistics show there is still much to be done for women with ovarian cancer and that there needs to be a clear and accessible understanding of the latest scientific advancements and novel therapies. At AstraZeneca we have focused our attention in this area. Our aim is to help improve the outcomes of these patients and our ambition is to one day eliminate cancer as a cause of death.
The functions of the ovaries – small but powerful
To understand ovarian cancer, we must first understand the evolving role of the ovaries. One function only starts at puberty; the ovaries secrete reproductive hormones, the most commonly known being oestrogen and progesterone, to drive the reproductive cycle and develop physical female characteristics. When a female goes through menopause, usually in her 40s or 50s, the ovaries stop producing as much oestrogen and no longer release an egg each month1,9,10 – the menstrual cycle stops.
The amount of hormone secreted therefore changes not only throughout the menstrual cycle but also across a lifespan. There is also disparity in ovarian cancer across the ages; although younger women can develop ovarian cancer, it usually affects women who have reached menopause5 with almost 80% of diagnoses being women aged 50 and above.5
Why is the survival rate still so low?
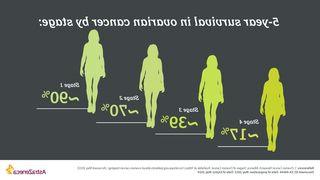
There’s a reassuring link between rapid diagnosis of ovarian cancer and improved survival.11,12,13,14 Cancer progresses through four stages of development, from early (stages 1-2) to late (stages 3-4) and once it has become ‘advanced’, it may have spread from the ovaries to other parts of the body and can be more challenging to control.8-11
Two thirds of women are currently diagnosed with late-stage disease, when the cancer has already spread beyond ovaries, making it harder to treat, and greatly reducing survival. Despite this clear correlation between rapid diagnosis and survival, most ovarian cancers are diagnosed at a late stage15,16,17 – but why?
Part of the complexity comes from recognising early symptoms so that the cancer can be diagnosed at an early stage. Symptoms are non-specific, meaning they can often go unnoticed or may be misdiagnosed for another illness until the cancer is advanced.17,20 It is important to remember that the four most common symptoms, listed here, may also not indicate the presence of cancer.

Another reason is that unlike other cancers, there is still no reliable and effective screening method for ovarian cancer,2,18 further delaying the ability to diagnose it. It is known that certain lifestyle19 and medical factors do indicate an increased risk of developing ovarian cancer which go beyond age, such as a lack of parity, endometriosis or a family history of ovarian, breast, or colorectal cancer.3,15,20 Beyond physical characteristics and lifestyle factors, a woman’s genetic makeup can also influence her risk of developing ovarian cancer…
Genetic pathways and gene mutations - have you HRD about them?
Every cell in the body suffers from DNA damage and undergoes a repair process in order to function normally.21 The Homologous Recombination Repair (HRR) pathway is just one genetic pathway which produces proteins, such as BRCA1/2, among others, to carry out this repair process via double-stranded breaks. PARPs (poly(ADP-Ribose) Polymerases) are an example of a family of enzymes vital to another genetic pathway, to repair single-stranded DNA breaks.21,22 This DNA damage response (DDR) shines a light on the connection between gene mutation and ovarian cancer.
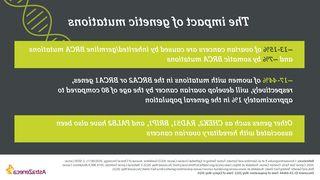
HRD stands for Homologous Recombination Deficiency, a lack of functional components in one or more of the DNA repair pathways and a common trait of cancer cells, which have a high genetic mutation rate. One example is BRCA. Both men and women possess BRCA1 and BRCA2 proteins which, when functioning normally, act as tumour suppressors.23 Their role within the HRR pathway is to repair cell damage and prevent them from growing and dividing too quickly – mutated BRCA genes result in abnormal cells which grow uncontrollably24 and are just one of many HRDs.
You can find out more about the DDR, HRD and other molecules involved here.
What is the importance of testing at diagnosis?
Genetic testing allows both clinicians and patients to make an informed decision when it comes to the treatment they receive. Conducting testing prior to or at the point of diagnosis can be important in improving patient care and enabling access to certain targeted therapies.25 By understanding the heritability of a woman’s cancer (if the mutation she possesses can be inherited) a patient’s family can also understand their risk of developing the disease – understanding the full picture has important implications for cancer risk assessment and prevention among relatives.26
What does this mean for treatment?
It’s one thing to know the link between genetic mutations and cancer development, another to leverage the science and target genetic vulnerability in order to optimise treatment. Targeted therapy for advanced ovarian cancer hinges on understanding the repair pathways and exploiting HRD by targeting PARPs. By inhibiting PARPs, the cells cannot repair single-stranded DNA breaks through its normal way and must rely on other pathways (such as HRR) to do so. Because cancer cells have HRD there are already fewer functional pathways; for BRCA mutations, there are fewer HRR pathways. This means cellular damage goes beyond the point of repair and results in cell death. Thus, the growth of abnormal cells is prevented.21

Our understanding of how to exploit HRD is evolving. We will continue our research in this pathway to further our understanding of how treatment options and combinations can potentially help achieve the best possible outcome.
Treatment falls into active and maintenance therapy. Active treatment includes surgery, chemotherapy and radiotherapy and maintenance therapy typically follows one round of active treatment. When a woman with ovarian cancer is in remission, she may have no treatment or otherwise undergo maintenance therapy to control the cancer.27,28 Age may influence such treatment options.29
Our approach
As leading pioneers, AstraZeneca has a portfolio of approved and potential treatment for advanced ovarian cancer including in newly diagnosed patients. Through our research, we have made progress in increasing the time that women can live without disease progression and improving quality of life. Our approach is based on using ground-breaking science to further our understanding of targeted therapy within ovarian cancer, focusing on patients with HRD and transferring our learnings to the wider patient population and paving the way to achieve the best possible outcomes for progression-free and overall survival.
Although progress has been made to understand the disease and novel therapies, there is still a very long way to go to expose the threat of ovarian cancer and help save more lives. Improvements in earlier diagnosis and accelerated access to the best available diagnostic testing and medicines are achievable goals which could help save countless lives.
Addressing the gaps in ovarian cancer care
As a founding member of the Ovarian Cancer Commitment (OCC), together with our partners European Society of Gynaecological Oncology (ESGO) and the European network of Gynaecological Cancer Advocacy Groups (ENGAGe) we have a bold ambition to improve the experience and survival of people living with ovarian cancer.

We are committed to working with communities and healthcare systems to help catalyse a change in the approach to diagnosing and managing ovarian cancer.
Our aim is to facilitate earlier interventions – including highlighting the importance of access to rapid diagnosis, genetic and biomarker testing and specialised care – and empower healthcare teams as they provide ongoing management and support for those living with this disease.
The OCC provides a platform for partners to pledge their commitment and implement tangible actions. We aim to increase membership of partner organisations as the initiative evolves, to reflect and address remaining gaps in the care of those with ovarian cancer across the globe.

References
- Livescience. Ovaries: Facts, Function and Disease. Available at http://www.livescience.com/58862-ovary-facts.html. Accessed May 2022.
- Patni R. Screening for Ovarian Cancer: An Update. Journal of Mid-Life Health. 2019;10(1), pp.3-5.
- Momenimovahed Z, et al. Ovarian cancer in the world: epidemiology and risk factors. International Journal of Women's Health. 2019;11:287-299.
- World Health Organization. IARC Estimated number of cases in 2018, worldwide, females, all ages. Available at http://gco.iarc.fr/today/. Accessed May 2022.
- OCRA. Recurrence. Available at http://ocrahope.org/patients/about-ovarian-cancer/recurrence/. Accessed May 2022.
- Chemoth. Explanation of First-line and Second-line Chemotherapy Regimens. Available at http://chemoth.com/firstline. Accessed May 2022.
- Chemoth. Evaluation of Chemotherapy Treatment. Available at http://chemoth.com/evaluation. Accessed May 2022.
- NHS Choices. 2020. Treatment Ovarian Cancer. Available at http://www.nhs.uk/conditions/ovarian-cancer/treatment/. Accessed May 2022.
- WebMD. 2021. Menopause? Available at http://www.webmd.com/menopause/guide/menopause-basics#:~:text=Their%20ovaries%20also%20make%20the,after%20the%20age%20of%2040. Accessed May 2022.
- NHS Choices (2018). Menopause Overview. Available at http://www.nhs.uk/conditions/menopause/. Accessed May 2022.
- Ovarian Cancer Research Alliance. About Stage I Ovarian Cancer. Available at ocrahope.org/patients/about-ovarian-cancer/staging/stage-1/. Accessed May 2022.
- Ovarian Cancer Research Alliance. About Stage II Ovarian Cancer. Available at ocrahope.org/patients/about-ovarian-cancer/staging/stage-2/. Accessed May 2022.
- Ovarian Cancer Research Alliance. About Stage III Ovarian Cancer. Available at ocrahope.org/patients/about-ovarian-cancer/staging/stage-3/. Accessed May 2022.
- Ovarian Cancer Research Alliance. About Stage IV Ovarian Cancer. Available at ocrahope.org/patients/about-ovarian-cancer/staging/stage-4/. Accessed May 2022.
- Target Ovarian. Key Facts and Figures. Available at http://targetovariancancer.org.uk/about-us/media-centre/key-facts-and-figures. Accessed May 2022.
- Cancer Research UK. Ovarian cancer statistics. Available at www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/ovarian-cancer/incidence#heading-Three. Accessed May 2022.
- Colombo N, et al. ESMO–ESGO consensus conference recommendations on ovarian cancer: pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Annals of Oncology. 2019;30:672-705.
- Cancer Research UK. Screening. Available at http://www.cancerresearchuk.org/about-cancer/ovarian-cancer/getting-diagnosed/screening. Accessed May 2022.
- Cancer.org. Ovarian Cancer Risk Factors. Available at http://www.cancer.org/cancer/ovarian-cancer/causes-risks-prevention/risk-factors.html. Accessed May 2022.
- World Ovarian Cancer Day. What is Ovarian Cancer? Available at http://www.cancer.gov/about-cancer/causes-prevention/genetics/brca-fact-sheet. Accessed May 2022.
- Bohen S, et al. DNA Damage Response –An Emerging Target for Groundbreaking Cancer Therapies. European Oncology & Haematology 2018;14(Suppl 1):2-7.
- Pascal J. The comings and goings of PARP-1 in response to DNA damage. DNA Repair. 2018;71:177–182.
- Bonadio R, et al. Homologous recombination deficiency in ovarian cancer: a review of its epidemiology and management. Clinics (Sao Paulo). 2018 Aug 20;73(suppl 1):e450s.
- Ovarian Cancer Action. What Are Genetic Mutations? Available at http://www.cancer.gov/about-cancer/causes-prevention/genetics/brca-fact-sheet. Accessed May 2022.
- Ngoi NYL, et al. The role of homologous recombination deficiency testing in ovarian cancer and its clinical implications: do we need it? ESMO Open Cancer Horizons 2021;6(3):1-12.
- National Cancer Institute. (2019). BRCA1 and BRCA 1: Cancer Risk and Genetic Testing. Available at http://www.cancer.gov/about-cancer/causes-prevention/genetics/brca-fact-sheet. Accessed May 2022.
- Force. Ovarian Cancer Treatment. Available at http://www.facingourrisk.org/understanding-brca-and-hboc/information/cancertreatment/ovarian-treatment/basics/maintenance-therapy-ovarian-cancer.php. Accessed May 2022.
- Cancer Council Queensland - Active Treatment. Available at http://cancerqld.org.au/glossary/active-treatment/. Accessed May 2022.
- Van Walree IC, et al. Treatment decision-making in elderly women with ovarian cancer: an age-based comparison. Int J Gynecol Cancer. 2019;29(1):158-165.