
Defining new targets in liver cancer
Home / Our therapy areas / Oncology / Liver Cancer
The liver performs numerous vital functions including filtering the body’s blood supply and – as a key organ of the immune and circulatory systems – contains numerous immune cells that defend the body against blood-borne pathogens and aid in wound healing.1,2,3,4 In addition, the liver is regenerative, meaning it can replace damaged tissue by regrowing its existing tissue – up to two-thirds of its total size.5,6,7 The unique pathogen-clearing and wound-healing properties of the liver require that resident immune cells are often active and ready to protect the body from harm.3,4 As part of this ability to protect the body, liver immune cells are typically also able to detect cells that have become abnormal, attacking and removing them before they can divide and grow into dangerous tumours.3,8 This state of immune readiness is a critical way liver immune cells are able to rapidly respond to pathogens and injury.9
Chronic inflammation – the “Achilles’ heel” of the liver
Inflammation is a natural part of the immune system’s standard reaction to threats.9 Ordinarily, inflammation is acute, or short term, and ends once a pathogen is removed or an injury is healed.9 But there are cases when the inflammatory response persists.10 Liver damage from hepatitis virus infection or as a result of excessive and prolonged alcohol intake can lead to chronic inflammation that ultimately may interfere with the typical ability of liver immune cells to attack and remove abnormal cells.10,11 When immune cells are hampered in this way, we call it immunosuppression.12 Unfortunately, immunosuppression in the liver can last even after the damaging period.5 With immune cells less able to attack and remove abnormal cells, cells in the liver are more likely to grow into cancer.11 Removing immunosuppression and restoring the ability of immune cells to attack and remove abnormal cells may be a key way to manage cancers that arise in the liver.11,13


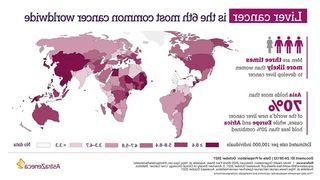
Liver cancer remains on the rise
For decades, the number of liver cancer cases globally have continued to rise.14 In 2020, liver cancer was the third most common cause of all cancer-related deaths.15* Hepatocellular carcinoma (HCC) is the most common form of liver cancer among adults, representing about 75% of all primary liver cancer cases.16,17
Why is liver cancer so prevalent?
Between 80 and 90% of HCC cases develop as a result of cirrhosis, the most common of which is infection with hepatitis B or C viruses.17 These viruses are widespread and challenging to manage, particularly in many developing parts of the world, making reducing the global burden of HCC difficult.18,19 More than 72% of the world’s HCC cases are found in Asia where these viruses are endemic.20-22 China alone accounts for more than half of all newly diagnosed liver cancer cases and deaths, despite containing less than 20% of the world’s population.23
Ongoing programs focused on prevention and screening of hepatitis are important to reduce the number of new HCC cases.17,18,19 However, there remains an urgent need for research that will provide more effective treatment options for patients with HCC than what is available today.24
Treating HCC
Screening for HCC is challenging.25 While early detection is the goal, most signs and symptoms appear when HCC is at an advanced stage, and early-stage tumours are often difficult to detect in a physical exam.25 As such, most patients are diagnosed at later stages of the disease when treatment options are limited.25
HCC is staged according to the Barcelona Clinic Liver Cancer (BCLC) system, with the disease stage determining what options are available to patients:26
Treatment for early stage (Stage 0 to A) disease and intermediate stage (Stage B) disease may involve:27,28
Surgery to remove the tumour.
Liver transplant may be a curative treatment for some patients with early stages of disease.
Thermal ablation (also referred to as radiofrequency ablation or microwave therapy) uses heat to destroy cancer cells in patients in the earliest stages of disease.
Transarterial chemoembolisation, or TACE is used to treat early- and intermediate-stage tumours that cannot be treated with surgery or thermal ablation. During the procedure, physicians deliver chemotherapy directly into the artery, which is then blocked to increase the tumour’s exposure to the medication.
Treatment for intermediate stage (Stage B) and advanced stage (Stage C) disease may involve:29
Systemic therapy is used in Stage B patients who are ineligible for other treatments or progressed on other therapies, as well as Stage C patients. There is a critical unmet medical need for new treatments that can treat patients with advanced stages of HCC. Ongoing research has revealed Immuno-Oncology therapies show promise in this challenging setting.
Our approach
Pioneering new research has deepened our understanding of the processes leading to the immunosuppression involved in liver cancer.13 Mounting evidence has shown that reversing immunosuppression may restore the ability of immune cells to attack and remove cancer cells, potentially slowing growth of or shrinking tumours.30
Treatment that reverses immunosuppression is called immunotherapy, and there are now multiple immunotherapies that may lead to anti-tumour activity.30,31 Our goal is to explore immunotherapy combinations for overcoming the drivers of immunosuppression involved in liver cancer, and with the aim of transforming survival for patients with liver cancer.
These efforts continue to build on the practice-changing results of our diverse, Immuno-Oncology clinical programme in multiple, solid tumours, and we remain committed to harnessing the versatile power of immunotherapy and immunotherapy combinations to redefine cancer care.
Our scientific platform
Immuno-oncology (IO)

Immunotherapies are designed to target immune checkpoints that are exploited by cancer to avoid or suppress the immune system’s ability to recognise and destroy cancer cells. Across our clinical trials, we are testing IO as monotherapy (by itself) and also in combinations with chemotherapy, small molecules, antibody drug conjugates and other immunotherapies across multiple tumour types, stages of disease and lines of treatment.
More about liver cancer

Other key disease areas
Join us
At AstraZeneca, we’re driven by innovation and our commitment to make a real-life difference in patients’ lives. Join us and help deliver life-changing medicines. Be among our employees who continue to make us an innovation-driven company that stands firmly among the world’s leaders in biopharmaceuticals.
Our people
"I believe personalised healthcare is the future of medicine; it allows us to use the latest diagnostic science to target medicines to patients most likely to benefit." Ruth March, Senior Vice-President of Precision Medicine, R&D Oncology



References
1. Naruse K, et al. Artificial and Bioartificial Liver Support: A Review of Perfusion Treatment for Hepatic Failure Patients. World J Gastroenterol. 2007;13(10):1516‐1521.
2. Cullen JM, et al. Liver and Biliary System. Jubb, Kennedy & Palmer's Pathology of Domestic Animals. 2016;2:258‐352.e1.
3. Endig J et al. Dual Role of the Adaptive Immune System in Liver Injury and Hepatocellular Carcinoma Development. Cancer Cell. 2016;30(2):308-323.
4. Krzyszczyk P, et al. The Role of Macrophages in Acute and Chronic Wound Healing and Interventions to Promote Pro-wound Healing Phenotypes. Front Physiol. 2018;9:419.
5. Markose D, et al. Immune Cell Regulation of Liver Regeneration and Repair. J Immunol Regen Med. 2018;2:1-10.
6. Kwon YJ, et al. Clinical Implications of Advances in Liver Regeneration. Clin Mol Hepatol. 2015;21(1):7-13.
7. Michalopoulos GK. Liver Regeneration. J Cell Physiol. 2007;213(2):286-300.
8. Eggert T, et al. Tumor Regulation of the Tissue Environment in the Liver. Pharmacol Ther. 2017;173:47‐57.
9. Robinson M, et al. Liver Immunology and its Role in Inflammation and Homeostasis. Cell Mol Immunol. 2016;13:267-276.
10. Tanaka M, et al. Liver Regeneration and Fibrosis after Inflammation. Inflamm Regener. 2016;36:19.
11. Kubes P, et al. Immune Responses in the Liver. Annu Rev Immunol. 2018;36:247-277.
12. Han Y, et al. Human CD14+ CTLA-4+ Regulatory Dendritic Cells Suppress T-Cell Response by Cytotoxic T-Lymphocyte Antigen-4-Dependent IL-10 and Indoleamine-2,3-Dioxygenase Production in Hepatocellular Carcinoma. Hepatology. 2014;59(2):567-579.
13. Lu C, et al. Current Perspectives on the Immunosuppressive Tumor Microenvironment in Hepatocellular Carcinoma: Challenges and Opportunities. Mol Cancer. 2019;18:130.
14. Altekruse SF, et al. Changing Hepatocellular Carcinoma Incidence and Liver Cancer Mortality Rates in the United States. Am J Gastroenterol. 2014;109(4):542‐553.
15. WHO International Agency for Research on Cancer. World. Available at: http://gco.iarc.fr/today/data/factsheets/populations/900-world-fact-sheets.pdf. Accessed May 2022.
16. ASCO. Liver Cancer: Introduction. Available at: http://www.cancer.net/cancer-types/liver-cancer/intro-duction. Accessed May 2022.
17. Li D, et al. Current Treatment Landscape for Advanced Hepatocellular Carcinoma: Patient Outcomes and the Impact on Quality of Life. Cancers (Basel). 2019;11(6):841.
18. Zampino R, et al. Hepatitis B Virus Burden in Developing Countries. World J Gastroenterol. 2015;21(42):11941‐11953.
19. Averhoff FM, et al. Global Burden of Hepatitis C: Considerations for Healthcare Providers in the United States. Clin Infect Dis. 2012;55 Suppl 1:S10‐S15.
20. Singal AG, et al. Epidemiology and Surveillance for Hepatocellular Carcinoma: New Trends. J Hepatol. 2020;72(2):250-261.
21. Petruzziello A, et al. Global Epidemiology of Hepatitis C Virus Infection: An Up-Date of the Distribution and Circulation of Hepatitis C Virus Genotypes. World J Gastroenterol. 2016;22(34):7824‐7840.
22. Shan S, et al. How to Control Highly Endemic Hepatitis B in Asia. Liver Int. 2018;38 Suppl 1:122‐125.
23. Zheng R, et al. Liver Cancer Incidence and Mortality in China: Temporal Trends and Projections to 2030. Chin J Cancer Res. 2018;30(6):571‐579.
24. Bupathi M, et al. Hepatocellular Carcinoma: Where There is Unmet Need. Molecular oncology. 2015;9(8):1501-1509.
25. American Cancer Society. Can Liver Cancer Be Found Early? Available at: http://www.cancer.org/cancer/liver-cancer/detection-diagnosis-staging/detection.html. Accessed May 2022.
26. Cancer Research UK. BCLC staging system and the Child-Pugh system. Available at: http://www.cancerresearchuk.org/about-cancer/liver-cancer/stages/bclc-staging-system-child-pugh-system. Accessed May 2022.
27. Vogel A, et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology. 2018;29(4):IV238-IV255.
28. ASCO. Embolisation Therapy for Liver Cancer. Available at: http://www.cancer.org/cancer/liver-cancer/treating/embolization-therapy.html. Accessed May 2022.
29. Kim E and Viatour P. Hepatocellular carcinoma: old friends and new tricks. Experimental & Molecular Medicine. 2020;52:1898-1907.
30. Joshi S, et al. Combinatorial Approach to Improve Cancer Immunotherapy: Rational Drug Design Strategy to Simultaneously Hit Multiple Targets to Kill Tumor Cells and to Activate the Immune System. J Oncol. 2019;2019:5245034.
31. National Cancer Institute. Immunotherapy to Treat Cancer. Available at: http://www.cancer.gov/about-cancer/treatment/types/immunotherapy. Accessed May 2022.
Veeva ID: Z4-42953
Date of prep: May 2022